
Summer 2016 The Future of Innovation in Medtech: An Industry in Search of Growth While Facing Pressures to Consolidate in a Post-ACA World By Cynthia Yee, Principal, Windham Venture Partners
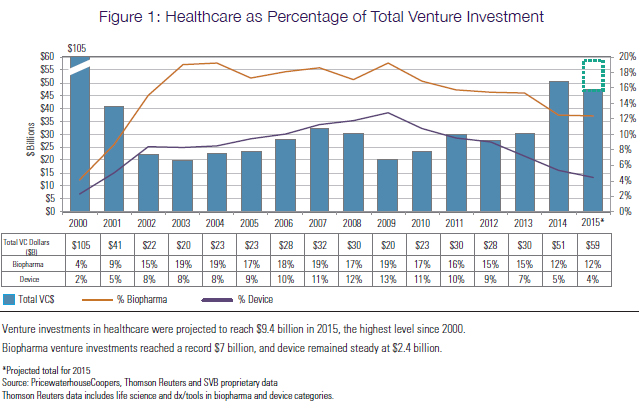
In the Affordable Care Act (ACA) era, the healthcare industry has witnessed significant consolidation among hospitals and commercial payers, which in turn has pressured big pharma and medical device manufacturers to consolidate in order to gain greater scale and improve their pricing and distribution leverage with providers. In recent years, some of the largest M&A transactions in healthcare—both in the pharmaceutical and medical device sectors—have been consolidation plays driven by the attractive financial synergies gained from increased operating leverage and, in many cases, non-domiciled tax advantages. This focus on operational scale and efficiency over innovation has been most pronounced in the medical device sector, which has faced a tough regulatory environment and increasing reimbursement pressures, as well as stagnant growth in mature end-markets. Under these pressures, naturally the medical device industry turned inward to drive profitability. The medtech sector has seen not only strategic M&A, but also institutional venture investment lag behind other healthcare sectors (see Figure 1 below) in aggregate and as a percent of total dollars invested, according to a report by Silicon Valley Bank (SVB) titled Trends in Healthcare Investments and Exits in 2016. According to SVB, declining investor interest in device[s] led to a drop in new company formation, with a more than 40 percent decline in deals and more than two-fold decrease in the total dollars invested in early-stage traditional medtech in 2015 compared to the prior five-year period.
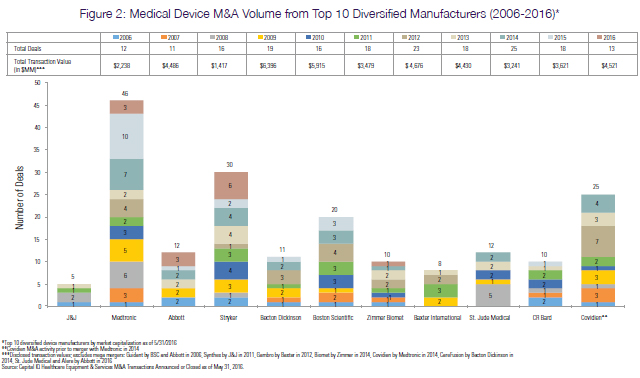
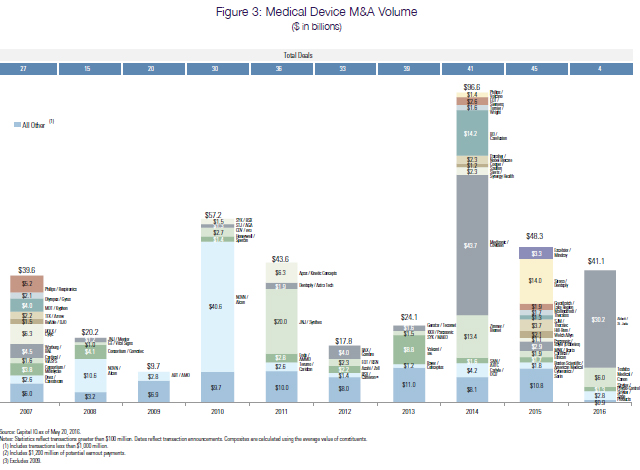
While more active corporate venture groups have helped to offset this funding gap, they have largely focused their dollars on later-stage assets or on companies in adjacent markets with complementary technologies that can easily tuck into existing infrastructure—the few notable exceptions being Abbott, Covidien, and Medtronic. Thus, with the recently announced union of Abbott and St. Jude Medical on the heels of the 2014 mega-merger between Medtronic and Covidien, entrepreneurs and investors are left wondering, Where does innovation-driven growth rank on the priority list of the largest medical device manufacturers? The 10 largest diversified medical device manufacturers in the U.S. have each demonstrated the ability to generate in excess of $1 billion in unlevered FCF annually and have record levels of cash on their balance sheets.1 In conjunction with interest rates on corporate debt at a historical low,2 strategics have significant financial flexibility to drive growth through investment in R&D or the acquisition of novel technologies. Nonetheless, R&D as a percent of total revenue has not changed materially in the last decade,3 while overall M&A has remained flat (see Figure 2 below). In fact, a closer look at M&A activity reveals a pick-up in synergy-driven acquisitions and divestitures among a broader group of medical device manufacturers (see Figure 3 below).
Has the medtech industry matured to the point that distribution leverage from consolidation and financial engineering through share-buybacks will be the main driver of profitability going forward, or do there still exist needle-moving opportunities in early-stage venture companies that can generate attractive long-term value for investors and strategics? As someone who has been in this industry for nearly a decade on all sides of the table, I am confident that there remain several attractive emerging growth opportunities in medtech. The next wave of growth can be seen in the transformative innovation taking place in the following three sectors: 1) neuromodulation for disease modification, 2) interventional device therapies for chronic diseases, and 3) next-generation sequencing for personalized medicine. 1) Neuromodulation for Disease Modification The field of neuromodulation has grown steadily over the last two decades, fueled by gradual uptake across several markets: spinal cord stimulation (SCS) and dorsal root ganglion (DRG) for pain management, deep brain stimulation (DBS) for various neurological disorders, and sacral and peripheral tibial nerve stimulation (SNS/PTNS) for urinary/fecal incontinence. However, neuromodulation is by no means a mature market, but rather a fairly nascent field with years of robust growth ahead. In fact, it is one of the fastest-growing sectors in the medical device industry, with global sales exceeding $3.5 billion in 2015 and projected to nearly double to $6.5 billion in 2020.4 There is significant opportunity for long-term market expansion, given that the total addressable market for neuromodulation remains highly underpenetrated across all approved indications, with the therapy often last in the continuum of care due to its invasiveness, disparate response rates, and cost. While the physiologic mechanism of action underlying neuromodulation has not been well characterized to date, there is emerging research that attributes its therapeutic benefit to afferent effects on systemic and local neuroplasticity, as well as semi-durable biochemical effects from the release of neurotransmitters. This new clinical understanding of neuromodulation could lead to improved efficacy that drives broader adoption for existing technologies and, importantly, reveal novel nerve targets and additional therapeutic indications. Two companies on the forefront of selective neuron modulation and bioelectronic medicine are SetPoint Medical and Circuit Therapeutics, which are pioneering precise physiologic nerve targets to mediate inflammatory diseases such as arthritis and correct vision impairment, respectively. In addition, we are seeing significant advancement in the field with technologies that address the invasiveness of neuromodulation through wireless powering and communication. Over the years, there have been various unsuccessful attempts to reduce the implant burden that is a major drawback of neuromodulation. More recently, StimWave and Neuspera Medical have begun making waves in the neuromodulation field with the development of miniaturized platforms leveraging proprietary methods of energy delivery based on far-field and mid-field energy transmission, eliminating the need for leads and a battery and thereby significantly reducing the implant size, risk of infection, and procedure time. The exciting prospects for this field are evidenced by the spate of recent financings for early-stage neuromodulation companies, including Cala Health, Cardionomic, and Neuspera Medical, as well as the spinout of Nuvectra from GreatBatch Medical, the success of Nevro in the public markets, and, notably, the creation of Action Potential Venture Capital, a strategic venture fund focused on bioelectronic medicines within GlaxoSmithKline to explore the use of neuromodulation as a more effective means of treating chronic diseases alongside or ahead of drug therapy. 2) Interventional Device Therapies for Chronic Diseases According to the CDC, chronic diseases such as heart failure, COPD, diabetes, and arthritis are the leading causes of death and disability in the U.S., with over 130 million adults—or approximately 50 percent of the adult population—diagnosed with one or more chronic health conditions, costing the U.S. more than $200 billion annually in direct medical expenses. With an increasing focus on value and cost-effectiveness, it is clear that current approaches to treating chronic diseases, which typically include long-term pharmacotherapy with multiple concomitant drugs, are simply unsustainable. In the past, medical devices have been relegated to second-line therapy after medical intervention had failed. However, there are several benefits to a one-time device intervention in chronic diseases, including improved efficacy, avoidance of side effects, and elimination of compliance issues associated with chronic drug regimens. In particular, device solutions have evolved from the days of stents and balloons to targeted therapies that are based on a physiologic insight garnered from real-world clinical surrogates with decades of safety observations. This, for example, was the premise of Ardian—an interventional device for hypertension that was acquired by Medtronic for $800 million plus earnouts—a valuation driven by having both traditional device manufacturers and pharmaceutical companies recognize the blockbuster potential of a one-time treatment for hypertension over chronic drug administration. The next wave of physiologic-guided device solutions to chronic diseases can be seen in several promising early-stage companies, including: Fractyl and Metavention, which are pursuing novel interventional approaches to treat diabetes through duodendal resurfacing and targeted metabolic modulation, respectively; Relievant Medsystems, which is addressing chronic low-back pain through targeted ablation of the basivertebral nerve; and Holaira and Gala Therapeutics, which are pursuing interventional pulmonary solutions for COPD and asthma. There are clearly myriad approaches to treating chronic diseases, and only time and clinical data will determine whether any are viable based on the ability to provide a durable clinical benefit without significant safety concerns. The winning device solutions will likely be targeted, minimally invasive interventions that leave no implant behind and, given the importance of health economics, will ideally fit into existing referral channels and be performed in an outpatient setting. Interventional devices offer an alternative that may ultimately prove a better solution for patients struggling to manage a chronic condition for which few drugs have had meaningful impact. 3) Next-Generation Sequencing as a Critical Component of Personalized Medicine Personalized medicine for early diagnosis and targeted therapy is poised to become the new paradigm of care in oncology. The global market for molecular diagnostics totaled roughly $6.0 billion in 2015 and is projected to exceed $9.3 billion in 2020, fueled by widespread adoption of personalized diagnostics.5 The accuracy, expediency, and cost of next-generation sequencing (NGS) has reached a point at which it is becoming accessible to individual patients on a clinical level to diagnose, determine course of treatment, and improve outcomes through early, non-invasive assessment of therapeutic response and recurrence. According to IMS Institute for Healthcare Informatics, expenditures on cancer drugs totaled $107 billion in 2015 and are projected to grow up to 10 percent annually, reaching $150 billion in 2020. As expensive targeted drugs and combination immuno-oncology therapies become more prevalent, diagnostics will play a more critical role in the management of cancer patients to optimize clinical outcomes and manage costs by leveraging genome analysis to screen for high-responders. While the competitive landscape in NGS-based diagnostics appears crowded with established players such as Illumina and Genomic Health, there are several earlier-stage companies—notably Personal Genome Diagnostics (PGDx) and 10x Genomics—that are poised to emerge as leaders enabling a new paradigm for oncology diagnostics. The broad adoption of NGS-based diagnostics has been hampered by fundamental challenges related to accuracy, clinical actionability, logistics, and reimbursement. PGDx and 10x are developing solutions to these clinical and market challenges with innovative, proprietary approaches to bioinformatics and workflow that equip local hospital labs with the technology to perform diagnostic evaluations for patients on a level that was formerly only accessible at world-class institutions. The future of oncology lies in targeted therapeutics and NGS-based diagnostics will play an integral part in ensuring patients are treated in a cost-effective manner. With billions of dollars on the balance sheets of the largest potential acquirers in the industry and relatively easy access to capital at low interest rates, Im hopeful that large diversified medical device manufacturers and enlightened pharmaceutical executives will see the value in investing in innovation. I certainly do.
1 CapIQ CY2006 to CY2015 unlevered FCF and cash. 2 Ernst & Young Credit Markets 2015-16: Analysis and opinions on global credit markets, Issue 3. 3 CapIQ R&D as percentage of Total Revenues CY2006 to CY2015. 4 MarketsandMarkets Neuromodulation report, July 2015. 5 MarketsandMarkets Molecular Diagnostics Market report, 2015. Consumer Digital Health Was Just the Beginning By Ted Kucklick, President and CTO, Cannuflow Inc. Anyone involved in the medical device industry is very aware of consumer and digital health. This is something that seemingly came out of nowhere around 2010, when the first Digital Health Summit was held at the Consumer Electronics Show in Las Vegas. Previously, digital health had just a few exhibitors in a corner of the South Hall of the Las Vegas Convention Center. This area has expanded rapidly with an entirely new ecosystem of players and investors new to the healthcare space, including AT&T, Verizon, and Qualcomm. Last year, 2016 Digital Health, Sports Tech, Mommy Tech, and so on took over roughly half of the Sands Convention Center. The digital health space has attracted somewhere between $35 billion and $45 billion in venture capital. This has spawned more than two dozen private IPO companies with over $100 million raised, such as Flatiron, Jawbone, Sotera, Zenefits, and 23andMe. Acquisitions include Misfit (to Fossil Group), Cardiomems, and Basis, while IPOs include Fitbit, Evolent, Teladoc, and Castlight. Many are companies that none of us had likely heard of just five years ago. This is the story of abundant technology, rapid growth, large-scale clinical need, and a quick succession of legislative changes packed into a very short amount of time. Terrified of the FDA When I attended my first CES in 2012, the nearly universal attitude of those making consumer health devices was to avoid the FDA. There were devices that measured wellness, but carefully steered clear of actually treating or diagnosing an actual disease. Some wanted the halo effect of a medical device without stepping over the line and actually being one. Some, like 23andMe, were rebuked by the FDA for crossing that line. This attitude has changed dramatically in just the past two or three years. The most recent CES featured panelists from the strategics you would expect, such as J&J, Medtronic, McKinsey, and Microsoft, as well as attendees from Stryker, Smith + Nephew, and Zimmer-Biomet. The level of sophistication and maturity of the companies in digital health was far greater than in years past. Forty-five billion dollars in investment can do that for you. Just Because We Can You have a supercomputer in your pocket. Really. In 2009, the top-selling handsets were Nokia, Samsung, and LG. Few were smartphones. Apple just barely cracked the top 10. In 2016, the top three are Samsung, Apple, and Huawei. Any decent smartphone available today for less than $500 has more computing power than a $32 million (inflation adjusted), 1980s-era Cray-2 with wireless and cloud connectivity not even dreamed of then, with an interface that a three-year-old can use. It is this abundant availability of computing horsepower that is making digital health possible. Now Apple has a watch clearly aimed at the digital health market with twice the computing power of its first iPhones. Companies like AliveCor have turned a smartphone into a fully functional EKG. Others have used the smartphone to run ultrasound, consumer-level EEG brain trainers (InteraXon Muse) and remote cardiac monitoring (InfoBionic). The other factor powering digital health is not as obvious. These are very recent developments that have dramatically lowered the cost of building and scaling a digital health company. Two of these are IaaS and PaaS, or infrastructure and platform as a service. This is where server and cloud services can be purchased off the shelf, without having to build it yourself. The Urge to Merge The urge to merge is the next not-so-obvious thing driving the digital health space. It has to do with the massive consolidation of hospitals into integrated health systems, or IHNs. These are mega-networks of formerly independent hospitals. The latest, Northwell, a merger of the Long Island Jewish Hospitals (LIJ) and Lenox Hill systems, has just become the largest private employer in New York state. Cleveland Clinic, which just purchased Akron General, has long been the largest employer in Northern Ohio, eclipsing the auto assembly manufacturers. Some of these systems are offering their own narrow-network insurance products. What this means is that these large systems are becoming massive consumers for population health data. One of the companies serving this need is Evolent Health, a spinoff of The Advisory Board consulting firm. Other companies servicing these consolidated systems are Validic, which offers ways to tie data collection devices to patient records, and Fitbit, which has begun to offer an enterprise-scale wellness platform to hospital systems to help mitigate lifestyle diseases with activity and exercise for population health. Patients are incentivized to use these wellness devices in exchange for preferential health insurance pricing. These consolidated health systems are very different customers than the individual hospitals with a KOL target customer surgeon of the past. Driving Out Costs Medicare and Medicaid reimbursement levels used to be considered the floor. Now, with the end of the Medicare sustainable growth rate (SGR) formula for the consolidated systems, they are the new normal. There may be more volume in terms of patients, but these will be at lower margins. Cleveland Clinic recently embarked on a system-wide cost-cutting program with a goal of being profitable at these new lower reimbursement levels, and cut $550 million of expense out of its system.1 Rural hospitals are under particular stress. Many of these are running on just weeks of cash, or have operating losses and do not have a local larger network to merge into. There is more need out there than the old manual and analog methods can keep up with. The old methods are entirely inadequate to solve the health problems of populations at the scale being demanded today. The Alphabet Soup of Data Collection As most know, the days of fee-for-service and relying on small numbers of well-insured patients to make your business work are over. Value is the new watchword. The federal government is currently implementing an alphabet soup of programs, from the Affordable Care Acts Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) to the new Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) law that was passed with bipartisan approval just one year ago, to alternative payment models (APMs) and so on. Some of these programs that are designed to get hospitals and doctors working together directly conflict with antitrust and Stark Law conflict-of-interest rules, and run the risk of triggering False Claims lawsuits.2 All of them require massive amounts of new data collection. This represents new opportunities for services and innovative business models where doctors and hospitals are treated as a single economic entity, rather than as separate ones. This also means fundamental changes in traditional sales models and physician/hospital/industry relationships. The new model for reimbursement is that 40 percent of Medicare payments will be graded on improved efficiency, preventing complications, and patient satisfaction. There are incentives for meeting these goals and definite penalties for not doing so. This transition from fee-for-service and volume to value and bundled payments is the top concern of over 65 percent of all hospital administrators. Digital health may have gotten its start with consumer wellness gadgets, but it has grown far beyond this in a very short period of time. The number of information technology devices that tackle serious healthcare issues has exploded. Some wellness wearables stay within the consumer space, like Misfit, acquired by the fashion watchmaker Fossil Group for $260 million, while others like Fitbit (which IPOed for a $4.1 billion valuation) are seriously pursuing the hospital enterprise space. Some of these opportunities represent familiar territory to those from the traditional medical device sector, but other elements are very unfamiliar and attract new investors and strategics from outside the traditional medical device ecosystem. There probably has never been a more exciting time to be in healthcarebut there has also never been a time that has become so unfamiliar so quickly and demanded such rapid adaptation.
1 Edmund Sabanegh, M.D., and Michael Phillips, M.D., presentation at Beckers Hospital Review 7th Annual Meeting, Chicago, April 2016. 2 Walter Eisner, Medicare Forces Hospitals to Violate Stark Law — or Lose Funding, Orthopedics This Week, February 26, 2016. Staying Out of Trouble When Making Promotional Claims for Dietary Supplements By David Hoffmeister, Partner (Palo Alto), and Charles Andres, Associate (Washington, D.C.) The Dietary Supplements Health and Education Act of 1994 (DHSEA) created a new class of U.S. Food and Drug Administration (FDA)-regulated products—dietary supplements. Dietary supplements fall within the regulatory sub-category of food and include, but are not limited to, vitamins, minerals, herbs, and other botanicals.1 Dietary supplements must be labeled as such, and must not be represented for use as a conventional food or as a sole item of a meal or the diet.2 Dietary supplements are big business. A recent estimate pegs the U.S. market for dietary supplements at over $35 billion annually.3 It has been speculated that the dietary supplement market is growing in part because consumers of dietary supplements view the purchase and consumption of dietary supplements as investing in themselves. Another reason for this growth is that getting onto the market with a dietary supplement is relatively easy, with no prior regulatory approval or clearance required. Manufacturers and distributors of dietary supplements are responsible for evaluating and ensuring the safety of their products before placing them on the market to ensure that they meet all DSHEA requirements and FDA regulations.4 Manufacturers are also responsible for ensuring that labeling claims are supported by competent and reliable scientific data, including, in many cases, generating clinical data to support marketing claims. Further, at least 75 days prior to placing a dietary supplement into commerce, manufacturers are required to notify the FDA of any new dietary ingredient (NDI) that: 1) is contained in the dietary supplement, and 2) was not marketed in the U.S. prior to October 15, 2004.5,6,7 After the 75-day waiting period, and absent action by the FDA, the NDI-containing dietary supplement may be placed into U.S. interstate commerce. However, the FDAs failure to respond to a notification does not guarantee that the FDA agrees the NDI is safe or efficacious.8 Promotional Labeling Claims There are a number of ways that dietary supplement makers can run afoul of the FDA rules. These include the following:
In this article, we focus on labeling claims, including advertising claims, and discuss how to help minimize the risk of FDA and Federal Trade Commission (FTC) actions when making dietary supplement labeling claims. Foremost among the ways to minimize the risk of FDA and FTC actions is to not make disease or disease treatment claims, either expressly or through implied messaging. Disease and Disease Treatment Claims Must Be Avoided Disease and disease treatment claims are not allowed within dietary supplement promotional labeling or advertisements. That is, dietary supplements cannot be marketed to diagnose, treat, cure or prevent any disease.13 Such claims misbrand the product, and subject both the product and the manufacturer to enforcement action by both the FDA and the FTC.14 A disease is defined as damage to an organ, part, structure, or system of the body such that it does not function properly (e.g., cardiovascular disease), or a state of health leading to such dysfunctioning (e.g., hypertension) . . .15 Diseases resulting from essential nutrient deficiencies (e.g., scurvy, pellagra) are excluded from this definition, which can allow dietary supplements to carry claims related to a nutrient deficiency disease as discussed below. The FDA uses a variety of criteria to determine whether a dietary supplement is making disease claims.16 While disease claims may not be made for dietary supplements, there are a variety of claims that may be made when appropriate criteria are met. Allowable Claims for Dietary Supplements There are a number of claims that—depending upon the facts, circumstances, and ingredient(s) in a dietary supplement—may appear in promotional labeling and advertisements. Representative claim types include: 1) structure/function claims; 2) claims of general well-being; 3) claims related to a nutrient deficiency disease; and 4) qualified health claims. For the structure/function claims, claims of general well-being, and claims related to a nutrient deficiency disease, there are three general requirements:
Structure/Function Claims Structure/function claims describe the role of a nutrient or dietary ingredient intended to affect the normal structure or function of the human body and may characterize the means by which a dietary supplement ingredient acts to maintain a normal structure or function.21 Such claims have historically appeared on the labels of dietary supplements. Examples include calcium builds strong bones and fiber maintains bowel regularity. The line between structure/function claims and disease claims is often not clear cut, and supplement manufacturers and distributors should consult with counsel to minimize the risk of putative structure/function claims in fact being disease claims. General Well-Being Claims General well-being claims describe general well-being from consumption of a nutrient or dietary ingredient. An example of a general well-being claim is makes you feel better. Claims Related to a Nutrient Deficiency Disease Claims related to a nutrient deficiency describe a benefit related to a nutrient deficiency disease (such as a connection between the lack of vitamin C and the development of scurvy), but such claims are allowed only if they also say how widespread the disease is in the United States,22 as this helps consumers make an informed purchasing decision. Qualified Health Claims Qualified health claims generally are not supported by data that meets the significant scientific agreement standard required for making a health claim for a traditional food.23 They require a disclaimer, which is why they are qualified health claims. Qualified health claims language must be worded (qualified) in such a way that consumers are not misled about the nature of the supporting science. For example, qualified health claims include, but are not limited to, claims that cover a possible relationship between:
Examples of qualified health claims include the following:
Because the language in qualified health claims may be off-putting to consumers, dietary supplement manufacturers and distributors should carefully weigh the pros and cons of petitioning for and using a qualified health claim on dietary supplement labeling. Dissemination of Publications, Articles, and Book Chapters Containing Discussions of Disease and Dietary Supplements Under Section 5 of the DSHEA, information about a dietary supplement, including a publication, article, or book chapter that discusses treatment of a disease with a dietary supplement, shall not be considered promotional labeling when used in connection with the sale of a dietary supplement under certain conditions. The publication may be used in connection with the sale of the dietary supplement, and not be considered labeling, if it:
Dietary Supplement Advertising Dietary supplement makers and distributors can also run afoul of the FTC because of claims made for the dietary supplement in advertising. While the FDA has primary responsibility for dietary supplement labeling, the FTC has primary responsibility for evaluating dietary supplement claims made in advertising.25 The FTC reviews dietary supplement claims made in advertising under the following criteria:
The FTC evaluates both express and implied claims. For example, a dietary supplement label could state that 90 percent of cardiologists regularly take the product. The FTC would evaluate the literal percentage claim for being truthful, non-misleading, and adequately substantiated. Using the same criteria, the FTC would also evaluate the implied claim that the product offers some heart benefit.27 According to the FTC, an advertisement can also be misleading if material information is omitted or not included in the promotion. For example, a supplement that claims to eliminate a mineral deficiency may be misleading for failing to include the qualifying information that less than 2 percent of the general population has the deficiency.28 Another area where advertising can be problematic is in clear and prominent disclosure. For example, consider a weight loss dietary supplement. There is adequate substantiation that the supplement can contribute to weight loss when used in conjunction with diet and exercise. Advertising with a banner headline that claims Lose 5 Pounds in 10 Days with a fine print disclosure at the bottom of the ad stating restricted calorie diet and regular exercise required would, according to the FTC, lack clear and prominent disclosure.29 Conclusion Improper dietary supplement labeling claims can cause manufacturers and distributors to run afoul of FDA rules and misbrand the product. Improper dietary supplement product claims—including objective product claims—made in advertising can result in action by the FTC. The FTC gives significant deference to the FDAs determination regarding whether there is adequate support for a health claim. Thus, if the FDA determines that a dietary supplement health claim is violative, the FTC is likely to find that the same health claim used in advertising is also violative. Dietary supplement manufacturers and distributors should consult with legal counsel to ensure that these and other risks are minimized before marketing and advertising any dietary supplement.
2 What is the difference between a dietary supplement and a conventional food? FDA, (2016), available at: http://www.fda.gov/AboutFDA/Transparency/Basics/ucm194357.htm, last accessed May 18, 2016. 3 Retail sales of vitamins & nutritional supplements in the United States from 2000 to 2017 (in billion U.S. dollars),* statista, (2016), available at: http://www.statista.com/statistics/235801/retail-sales-of-vitamins-and-nutritional-supplements-in-the-us/, last accessed May 18, 2016. 4 See, e.g., Dietary Supplements, FDA, (2016), available at: http://www.fda.gov/Food/DietarySupplements/, last accessed May 17, 2016. 6 Notification must be given at least 75 days before the introduction of the NDI-containing supplement into the marketplace. The NDI may not be introduced into interstate commerce for 75 days after the FDA receives the NDI notification. 7 There is no authoritative list of dietary ingredients that were marketed in dietary supplements before October 15, 1994. Therefore, manufacturers and distributors are responsible for determining whether an ingredient is a new dietary ingredient. 9 For example, one way a dietary supplement can be adulterated is for the dietary supplement to contain a prescription drug. 10 To distinguish dietary supplements from conventional foods, look at the product nutrition label. Conventional foods must have a Nutrition Facts panel on their labels, but dietary supplements must have a Supplement Facts panel. 11 See The Food Allergen Labeling and Consumer Protection Act of 2004. The major food allergens include milk, eggs, fish, crustacean shellfish, tree nuts, peanuts, wheat, and soybeans. 12 A label is any display of written, printed, or graphic matter on the immediate container of any article, or any such matter affixed to any consumer commodity or affixed to or appearing upon a package containing any consumer commodity . . . 21 C.F.R. § 1.3(b). The term labeling means all labels and other written, printed, or graphic matter (1) upon any article or any of its containers or wrappers, or (2) accompanying such article. 21 C.F.R. § 321(m). Labeling includes most, if not all, advertising. 13 21 C.F.R. § 101.93(a)(3)(c). 14 See, e.g., 21 U.S.C. §§ 343 and 352. 16 See 21 C.F.R. § 101.93(g)(2)(i)-(x). 17 See, e.g., Guidance for Industry: Substantiation for Dietary Supplement Claims Made Under Section 403(r)(6) of the Federal Food, Drug, and Cosmetic Act, FDA, (2015), available at: http://www.fda.gov/food/guidanceregulation/guidancedocumentsregulatoryinformation/ 18 The FDA reviews notifications to ensure they meet the definition of a structure/function claim. If not, the FDA sends a letter to the manufacturer providing notification that the claim is not in compliance and follows up as needed. The FDA keeps copies of all notifications on file. 19 See, e.g., Guidance for Industry: Structure/Function Claims, Small Entity Compliance Guide, FDA, (2015), available at: http://www.fda.gov/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/ 20 E.g., This statement has not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease. 21 Label Claims for Conventional Foods and Dietary Supplements, FDA, (2016), available at: http://www.fda.gov/Food/IngredientsPackagingLabeling/LabelingNutrition/ucm111447.htm, last accessed May 17, 2016 (emphasis added). 22 Structure/Function Claims, FDA, (2016), available at: http://www.fda.gov/Food/IngredientsPackagingLabeling/LabelingNutrition/ucm2006881.htm, last accessed May 18, 2016. 23 See, e.g., 21 C.F.R. § 101.14. 24 Summary of Qualified Health Claims Subject to Enforcement Discretion, FDA, (2014), available at: http://www.fda.gov/Food/IngredientsPackagingLabeling/LabelingNutrition/ucm073992.htm, last accessed May 18, 2016. 25 See, e.g., FTC Act, §§ 5, 12, and 15. 26 Dietary Supplements: An Advertising Guide for Industry, FTC, (2001), available at: http://www.fda.gov/Food/GuidanceRegulation/GuidanceDocumentsRegulatoryInformation/ 27 In evaluating whether a claim is adequately substantiated, the FTC considers a number of factors, including: the type of product, the type of claim, the benefits of a truthful claim, the cost/feasibility of developing claim substantiation, the consequences of a false claim, and the amount of substantiation that experts believe is reasonable. 28 Id. at 5. See also Claims Related to a Nutrient Deficiency Disorder, supra. Life Sciences Venture Financings for WSGR Clients By Scott Murano (Partner, Palo Alto)
The data generally demonstrates that venture financing activity increased during the second half of 2015 compared to the first half of 2015 with respect to the total amount raised, but decreased with respect to the number of closings. Specifically, the total amount raised across all industry segments increased 8.5 percent from the first half of 2015 to the second half of 2015, from $576.66 million to $625.83 million, while the total number of closings across all industry segments decreased 14.5 percent, from 76 closings to 65 closings. Notably, the industry segment with the largest number of closings—medical devices and equipment—experienced a decrease in number of closings and in total amount raised during the second half of 2015 compared to the first half of 2015. Specifically, medical devices and equipment decreased 34.1 percent in number of closings, from 41 closings to 27 closings, and decreased 29.6 percent in total amount raised, from $306.32 million to $215.73 million. Conversely, the industry segment with the second-largest number of closings—biopharmaceuticals—experienced an increase in number of closings and in total amount raised during the second half of 2015 compared to the first half of 2015. Specifically, the number of closings in the biopharmaceuticals segment increased 5.3 percent, from 19 closings to 20 closings, and the total amount raised increased 29.5 percent, from $139.93 million to $181.21 million. Meanwhile, the industry segment with the third-largest number of closings—digital health—experienced an increase in number of closings and in total amount raised during the second half of 2015. Specifically, digital health experienced a 16.7 percent increase in number of closings, from six closings to seven closings, and a 228 percent increase in total amount raised, from $20.07 million to $65.83 million. All remaining industry segments—genomics, diagnostics, and healthcare services—were flat or marginally up in number of closings during the second half of 2015 and experienced an increase in total amount raised. Specifically, genomics increased 154.2 percent in total amount raised, from $12.84 million to $32.64 million; diagnostics increased 247.6 percent, from $9.5 million to $33.02 million; and healthcare services increased 10.7 percent, from $88 million to $97.4 million. In addition, our data suggests that Series A financing and bridge financing activity compared to Series B and later-stage equity financings and recapitalization financings decreased during the second half of 2015 compared to the first half of 2015. Specifically, the number of Series A closings as a percentage of all closings decreased from 37.2 percent to 29.2 percent, while the number of bridge financing closings as a percentage of all closings decreased from 30.8 percent to 26.2 percent. Offsetting those gains, Series B financing, Series C and later-stage financing, and recapitalization financing activity compared to all other financings decreased during the second half of 2015. The number of Series B closings as a percentage of all closings increased from 15.4 percent to 18.5 percent, the number of Series C and later-stage financing closings as a percentage of all closings increased from 10.3 percent to 21.5 percent, and the number of recapitalization financing closings as a percentage of all closings increased from 2.6 percent to 4.6 percent. Average pre-money valuations for life sciences companies increased for Series A financings but decreased at later stages of financing during the second half of 2015 compared to the first half of 2015. The average pre-money valuation for Series A financings increased 157 percent, from $8.57 million to $22.04 million; the average pre-money valuation for Series B financings decreased 26.2 percent, from $47.91 million to $35.36 million; and the average pre-money valuation for Series C and later-stage financings decreased 22.7 percent, from $108.75 million to $84.07 million. Other data taken from transactions in which all firm clients participated in the second half of 2015 suggests that life sciences is the second-most attractive industry for investment, up from third during the first half of 2015. For the second half of 2015, life sciences represented 14 percent of total funds raised, while the software industry—historically and still the most popular industry for investment—represented 36 percent of total funds raised. Services came in third, representing 13 percent of total funds raised. Overall, the data indicates that access to venture capital for the life sciences industry marginally increased during the second half of 2015 compared to the first half of 2015. The total amount raised has improved, but deal activity in terms of number of closings has declined, suggesting that deals remain difficult to come by. For those companies that are able to close on financing, the spread of average pre-money valuations at the different stages of financing has condensed, suggesting that companies may be forced to wait longer and demonstrate more value to investors before raising the first round of equity financing. It is also worth noting that financing activity during both the first half of 2015 and the second half of 2014 had decreased from their respective prior six-month periods, so the improved financing activity during the second half of 2015 is a welcome change and hopefully a sign of more to come.
Recent Life Sciences Client Highlights
China Biologic Completes $308 Million Follow-On Offering 24th Annual Medical Device Conference Phoenix 2016: The Medical Device and Diagnostic Conference for CEOs
Click here for a printable version of The Life Sciences Report This communication is provided as a service to our clients and friends and is for informational purposes only. It is not intended to create an attorney-client relationship or constitute an advertisement, a solicitation, or professional advice as to any particular situation. © 2016 Wilson Sonsini Goodrich & Rosati, Professional Corporation |
 Cynthia Yee is a Principal at Windham Venture Partners, a multi-stage healthcare venture capital firm based in New York and San Francisco. She was previously an equity research analyst at Piper Jaffray, a member of the healthcare investing team at New Enterprise Associates, and responsible for marketing and business development at Advanced Cardiac Therapeutics, a venture-backed medical device company.
Cynthia Yee is a Principal at Windham Venture Partners, a multi-stage healthcare venture capital firm based in New York and San Francisco. She was previously an equity research analyst at Piper Jaffray, a member of the healthcare investing team at New Enterprise Associates, and responsible for marketing and business development at Advanced Cardiac Therapeutics, a venture-backed medical device company. Ted Kucklick is co-founder, CEO, and CTO of Cannuflow, Inc., which is dedicated to developing innovative technologies for arthroscopic surgery. He has worked in R&D of innovative medical devices for numerous companies, including RITA Medical (acquired by ANGO), AfX, (acquired by Guidant), Somnus (acquired by Smith and Nephew), Sleep Solutions (now Novasom), and Starion Instruments (acquired by Pentax). Ted has a degree in product design and a certificate from the UC Berkeley Haas School of Business Global Bio-Entrepreneur program, and is a member of the IEEE/EMBS, AMI, and SME professional societies. He is also an inventor on over 61 issued patents.
Ted Kucklick is co-founder, CEO, and CTO of Cannuflow, Inc., which is dedicated to developing innovative technologies for arthroscopic surgery. He has worked in R&D of innovative medical devices for numerous companies, including RITA Medical (acquired by ANGO), AfX, (acquired by Guidant), Somnus (acquired by Smith and Nephew), Sleep Solutions (now Novasom), and Starion Instruments (acquired by Pentax). Ted has a degree in product design and a certificate from the UC Berkeley Haas School of Business Global Bio-Entrepreneur program, and is a member of the IEEE/EMBS, AMI, and SME professional societies. He is also an inventor on over 61 issued patents. 






